
Toxoplama gondii is ubiquitous in nature and infects animals and human alike. In immunocompetent host the infection is typically asymptomatic; however, in congenital settings, toxoplasmosis causes a range of manifestations in the fetus and newborn including but not limited to prematurity, IUGR, microcephaly, seizures, myocarditis, and life-long neurological and ophthalmologic sequelae.
The global incidence of congenital toxoplasmosis has been estimated to be 190,100 cases annually which corresponds to a burden of 1.20 million disability-adjusted life years. Yet only a few countries in the world have policies about universal serologic screening during gestation, followed by treatment of women who seroconvert.
Surprisingly, In USA, serological screening is not universally recommended, although some obstetric practices do the screening. The current issue of American Journal of Obstetrics and Gynecology reports the results of first RCT Toxogest (ClinicalTrials.gov Identifier: NCT01189448) compare the efficacy and tolerance of pyrimethamine + sulfadiazine(PS) vs spiramycin to reduce placental transmission with an accompanying editorial about the systematic screening of toxoplasmosis during pregnancy.
Since placebo-controlled RCT was not possible, the trial compared the potential of spiramycin vs. PS to treat congenital toxoplasmosis in 150 women who have seroconverted during their second trimester of gestation or later.
Unfortunately, the trial was terminated early because of insufficient participants and problems with funds, but there were fewer transmission and no fetal cerebral toxoplasmosis lesions in the PS group, prompting to perform further research on prevention of congenital toxoplasmosis.
However, there is a lot to learn from results of Toxogest trial write Jose G. Montoya from Department of Medicine, Division of Infectious Diseases and Geographic Medicine, Stanford University School of Medicine, Stanford, CA in the accompanying editorial.
Based on results of study and literature review so far, the author advises systematic screening for toxoplasmosis in every pregnant woman where Toxoplasma infection is known to occur because of devastating consequences of congenital toxoplasmosis. Further, congenital toxoplasmosis is preventable and treatable in utero.
If a woman tests positive or seroconverts during pregnancy, the question is not about to treat or not to treat, but what to treat with. The author proposed a simple algorithm for serological screening and follow up of pregnant women who were identified to be at risk for seroconversion during gestation (negative for Toxoplasma immunoglobulin G and M).

If Toxoplasma IgM/IgG remains negative along with normal fetal ultrasound till term, no further treatment is needed. If the patient seroconverts and tests positive for IgM/IgG, follow the following algorithm.

At 18 weeks of pregnancy, do amniotic fluid PCR in patients on Spiramycin or pyrimethamine +sulfadiazine(PS) and follow the algorithm.
The author concludes, “It is time to not leave anymore pregnant women who silently seroconvert for toxoplasmosis during gestation in the equivalence of a placebo arm.”
Ob/Gyn Updated Facebook page

If Toxoplasma IgM/IgG remains negative along with normal fetal ultrasound till term, no further treatment is needed. If the patient seroconverts and tests positive for IgM/IgG, follow the following algorithm.

At 18 weeks of pregnancy, do amniotic fluid PCR in patients on Spiramycin or pyrimethamine +sulfadiazine(PS) and follow the algorithm.
 |
| Algorithm after amniotic fluid PCR in Spiramycin group |
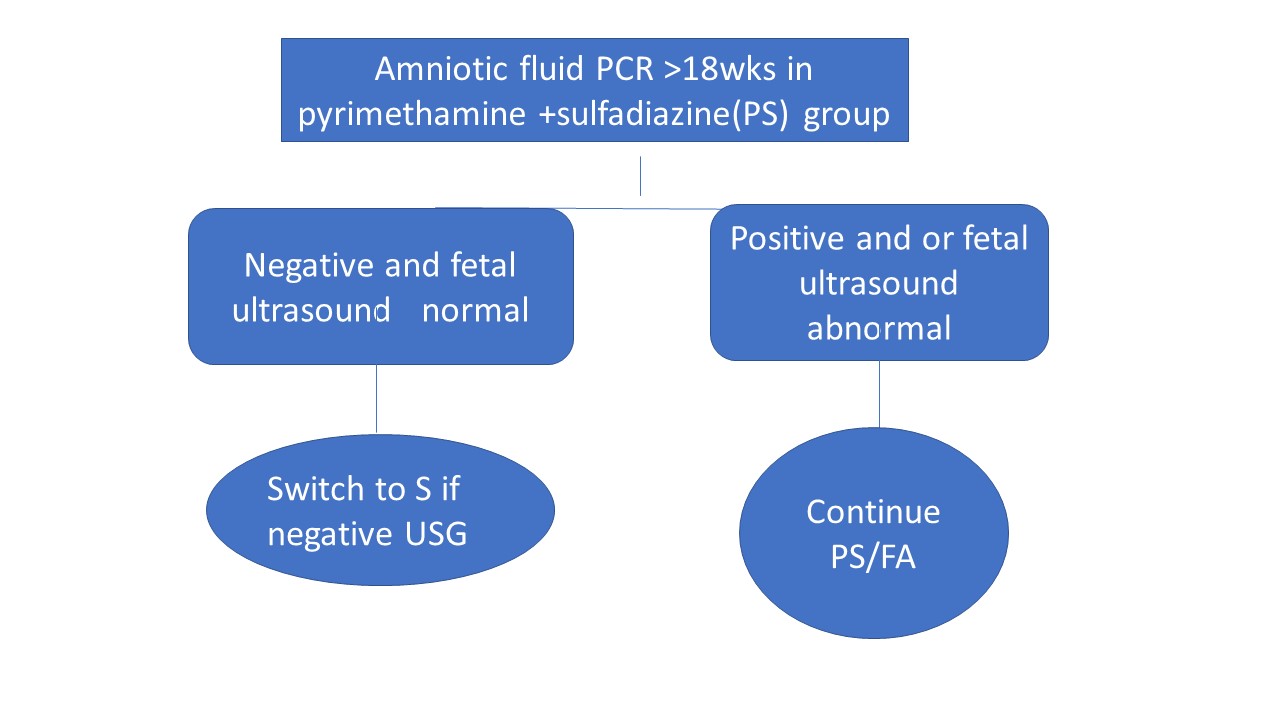 |
| Algorithm after amniotic fluid PCR in pyrimethamine +sulfadiazine(PS) group |
Ob/Gyn Updated Facebook page