Zika Virus was first isolated from rhesus monkeys in Zika forest in Uganda in 1947, but was barely in
news till now as it did not cause outbreak in humans.
The Zika virus is a flavivirus, part of the same family as
yellow fever, West Nile, chikungunya and
dengue. But unlike some of those viruses, there is no vaccine to prevent Zika
or medicine to treat the infection.
The incubation period of Zika virus disease is not clear,
but is likely to be a few days. The symptoms are similar to other arbovirus
infections such as dengue, and include fever, skin rashes, conjunctivitis,
muscle and joint pain, malaise, and headache. These symptoms are usually mild
and last for 2-7 days. But, majority of patients with this infection have no or
very little symptoms, causing it very difficult to track. They can, however,
still transmit the disease if they are bitten by a mosquito that then bites
someone else.
Transmission
The Vector for Zika is
Aedes mosquitoes (which usually bite during the morning and late
afternoon/evening hours. On Tuesday CDC reported the first sexually transmitted
case of Zika virus in Dallas,
Texas.
Previously, there have been only two
documented
cases linking Zika to sex and isolated cases of spread through blood
transfusion.
Diagnosis
According to CDC- During the first week of illness, Zika
virus disease can often be diagnosed by performing reverse
transcriptase-polymerase chain reaction (RT-PCR) on serum. Serology assays can
also be used to detect Zika virus-specific IgM and neutralizing antibodies,
which typically develop toward the end of the first week of illness. Plaque-reduction
neutralization testing (PRNT) can be performed to measure virus-specific
neutralizing antibodies to confirm primary flavivirus infections and
differentiate from other viral illnesses.
World Health Organization Director-General Margaret Chan
declared the current outbreak as
a public health emergency on February 1,
2016, with 24 countries involved from South and Central America and the Caribbean involved in the outbreak.
 |
| Courtesy: Vox.com |
Zika is commanding attention worldwide because of connection
between the virus and microcephaly.
According to CDC, in the past four months, microcephaly cases in Brazil rocketed
to 3,500 from 147, the average for the same time last year (2014). About
46 babies have died due to birth defects.
The link was first detected when Brazilian health authorities found traces
of the Zika virus in a deceased infant born with microcephaly or in amniotic
fluid of mothers delivering microcephalic infants.
The first confirmed cases of ZIKV infection in Brazil were reported in May 2015.
Transmission of the virus in Brazil
is likely to have started several months before because the disease is new and
mild, and could have been unrecognised or misdiagnosed, as dengue and
chikungunya epidemics were ongoing.
Microcephaly caused due to any infection is usually caused by transplacental
infections occurring early in pregnancy and is only detected during the second
half of pregnancy or after birth.
The observed six months delay between the recognition of the transmission of
ZIKV in May 2015, and the detection of an increase in microcephaly in November
2015, is therefore compatible with a temporal association between the two
events.
Currently there is only ecological evidence of an association between the
two events, due to sudden epidemic of microcephalic babies born and clustered
around a specific time period. Researchers are still working to confirm the
link — could it be something else that's causing the microcephaly?
On 13 January 2016, the Brazil Ministry of
Health reported the detection of Zika virus genome, through the RT-PCR
technique in four cases of congenital malformation in the state of Rio Grande do Norte. The
cases correspond to two miscarriages and two full-term newborns (37 and 42
weeks respectively) who died in the first 24 hours of life. Tissue samples from
both newborns were also positive for Zika virus by immunohistochemistry
Obstetrical providers should obtain a travel history from all pregnant women
and use recent travel history to guide decisions about testing. Testing
is not indicated for pregnant women without a travel history to an area with
Zika virus transmission.
 |
| Courtesy: Vox.com |
Diagnosis in pregnant patients.
Zika virus RT-PCR can also be performed on amniotic
fluid. Other testing that can performed includes the following: 1)
histopathologic examination and immunohistochemical staining of the placenta
and umbilical cord, 2) Zika virus testing of frozen placental tissue and cord
tissue, and 3) IgM and neutralizing antibody testing of cord blood.
Amniocentesis should be offered to pregnant women with
recent travel to an area with Zika virus transmission, reporting 2 or more
symptoms within two weeks of travel and a positive or inconclusive maternal
serum test. For pregnant women with recent travel to an area with Zika
virus transmission and ultrasound findings of microcephaly or intracranial
calcifications, amniocentesis may also be considered.
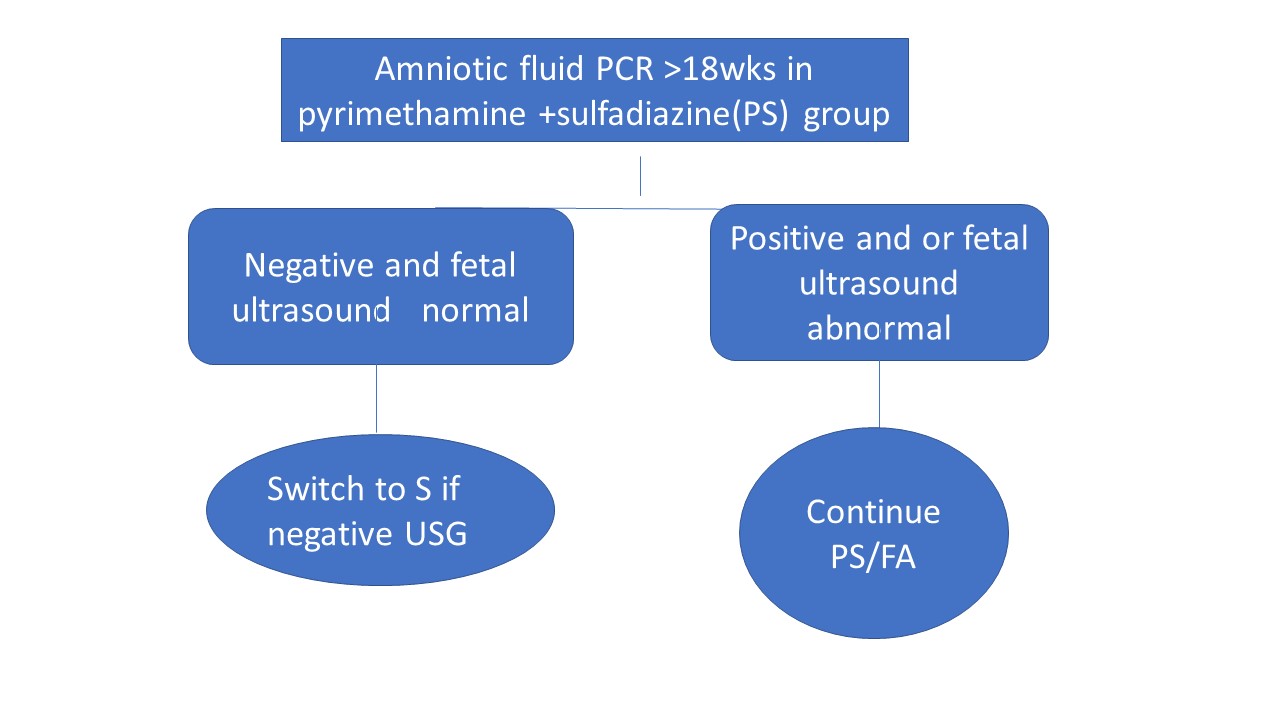
A positive Zika virus RT-PCR result from amniotic fluid
would be suggestive of intrauterine infection. This information would be
useful for pregnant women and their healthcare providers to assist in
determining clinical management (e.g., antepartum testing, delivery
planning). A negative Zika virus RT-PCR result from amniotic fluid may
prompt a work up for other causes of microcephaly (e.g., other infections,
genetic disorders).
There is currently no cure
for the Zika virus. A number of institutions are scrambling to develop
a vaccine, but it could take up to five years, as
health experts called for new incentives for drug companies.
References:
http://www.paho.org/hq/index.php?%20option=com_topics&view=article&id=427&Itemid=41484&lang=en